
Hip Pain: Symptoms, Causes, Treatment and When to See a Physio

What is Hip Pain?
Hip pain refers to discomfort, stiffness, or aching around the hip joint, groin, buttock, or outer thigh. It can result from inflammation, muscle strain, joint irritation, or referred pain from the lower back or pelvis.
A hip pain physio will assess the joints, muscles, and movement patterns around your hip to determine which structures are affected — then design a tailored plan to restore smooth, pain‑free movement.
Main Types of Hip Pain
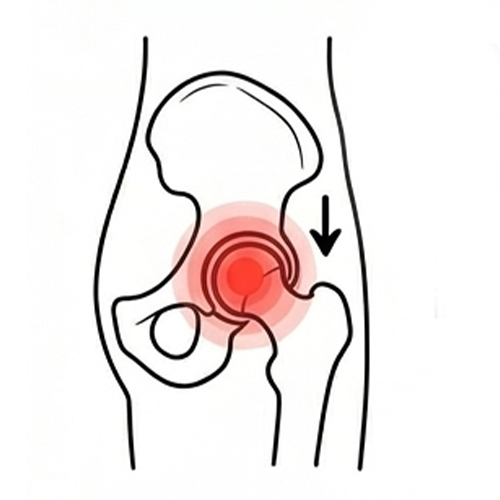
Groin Pain or Hip Joint Arthritis
Common in active adults or older individuals, felt deep in the front of the hip.
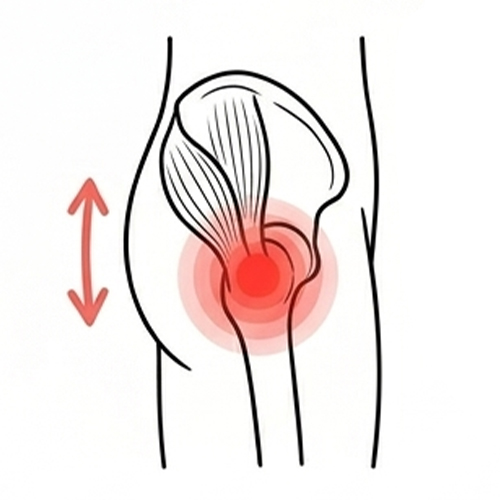
Gluteal or Outer Hip Pain (Trochanteric Bursitis)
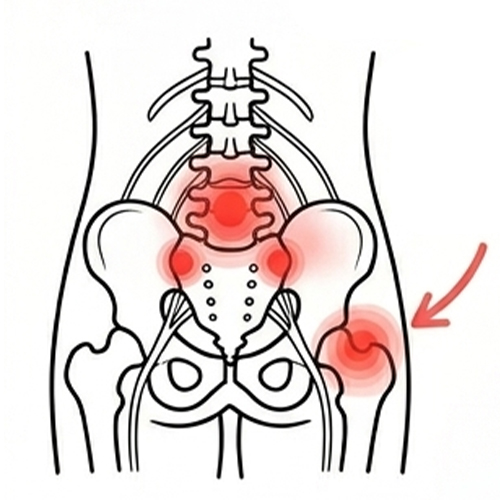
Referred Hip Pain from the Lower Back or SIJ
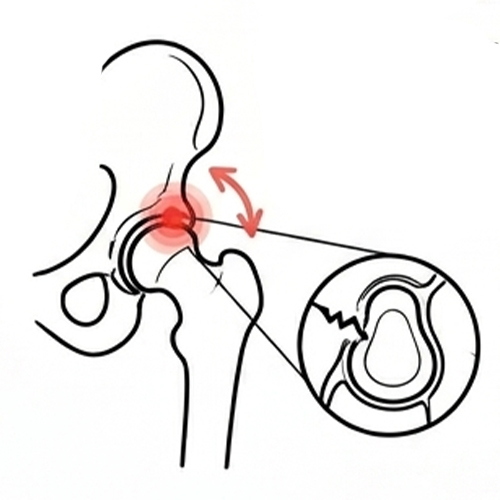
Labral Tear or Hip Impingement
Postural or Muscle‑Related Pain

Post‑Injury or Post‑Surgery Pain
Recovery challenges following trauma, fracture, or hip replacement surgery.
Common Causes and Contributing Factors
- Overuse or repetitive strain from sport or exercise
- Prolonged sitting or poor posture
- Weak glutes and core muscles
- Muscular imbalance or tight hip flexors
- Previous injury or hip impingement
- Stress or lifestyle factors increasing muscle tension
Often, hip pain develops from several small factors rather than one major event —
poor posture, weakness, and movement habits can interact to overload the joint
over time. Hip pain can overlap with pelvic discomfort. Pelvis pain physiotherapy in London may help.
Symptoms and What They Mean
Neck pain symptoms can vary widely depending on the structures involved:
- Dull, aching pain deep in the hip or groin
- Sharp pain when walking, climbing stairs, or sitting
- Stiffness after rest or first thing in the morning
- Clicking or locking sensations in the hip joint
- Pain lying on the affected side
- Weakness or difficulty squatting, running, or lifting
How Long Does Hip Pain Last?
Acute hip pain (less than 6 weeks) may settle quickly with physiotherapy, activity modification, and targeted exercises.
Sub‑acute pain (6–12 weeks) often requires a structured strengthening programme to restore function.
Chronic hip pain (12+ weeks) usually benefits from an integrated plan combining manual therapy, exercise, and movement retraining to reduce sensitivity and improve long‑term stability.
Getting help early prevents compensations that can lead to longer recovery times.
When Hip Pain Needs Urgent Attention (Red Flags)
Most hip pain is mechanical and responds well to physiotherapy, but urgent medical review is needed if you experience:
- Sudden inability to walk or bear weight after trauma
- Severe pain or swelling in the hip or thigh
- Numbness or tingling around the groin or leg
- Loss of bladder or bowel control
- Unexplained fever, weight loss, or night pain
How Physiotherapists Diagnose Hip Pain
- Take a detailed history of symptoms, lifestyle, and activity levels
- Inspect posture and movement patterns
- Test muscle strength, flexibility, and hip joint mobility
- Identify whether symptoms come from the hip, spine, or pelvic joint
- Use precise tests to rule out serious pathology
If imaging such as an X‑ray, ultrasound, or MRI is needed, your physiotherapist will coordinate with your GP or orthopaedic specialist to ensure continuity of care.
Physiotherapy Treatment for Hip Pain
Treatment may include:
Hands‑On Therapy
Exercise Therapy
Movement Retraining
Rehabilitation Programmes
How Physiotherapy Helps Long Term
- Restore joint range of motion and muscle balance
- Reduce inflammation and stiffness
- Improve posture and walking mechanics
- Support safe return to exercise, sport, or daily activity
- Prevent recurrence through education and movement trainin
Your hip pain physiotherapist will also teach you how to self‑manage symptoms and maintain strength, building resilience for the long term
When to See a Physio
- Pain persists beyond a few days or recurs frequently
- Sleep is disrupted by hip discomfort
- Pain limits walking, gym training, or daily activities
- You’re unsure whether exercise might worsen it
- Over‑the‑counter medication isn’t providing lasting relief
Take the Next Step Toward Recovery
At One Body, our physiotherapists specialise in hip pain treatment — from simple muscle tightness to complex hip impingement or post‑surgical rehab. We combine advanced assessment techniques, hands‑on therapy, and tailored rehabilitation so you can move confidently again without pain holding you back.
Learn more about hip pain

This page has been medically reviewed by Rebecca Bossick, Lead Clinical Physiotherapist, HCPC & CSP Registered.